
Lucky, a feisty little white female Maltese, had a pretty bad day on Thursday the 9th of June. She was hanging out at home being inquisitive and guarding the home base when she tipped her luck too far and fell out of the window. Dropping two floors onto a hard surface causing spinal cord damage and immediate paralysis from the neck down. Vicky, her Mum, rushed her to their vet Dr Deborah Jones at the Kohimarama Veterinary Clinic for emergency care. A decision was made to refer her to VSA for surgical assessment.
Lucky was seen by Dr Richard Jerram who localised the spinal damage to C1-5 (cervical 1 through to 5) and recommended a CT of that area of the spine. Lucky was in a lot of pain but could feel and move her legs and had normal mental awareness.
The CT was read by Dr Angela Hartmann and showed “a comminuted fracture associated with the occipital bone and basioccipital bone. This has likely resulted in atlantooccipital instability given that both occipital condyles are involved. There is at least one large segmental fracture associated with the right caudal portion of the occiput. No intracalvarial hemorrhage is noted.” This means that Lucky had probably landed on her head and the spinal vertebrae had pistoned into the back of her skull fracturing the bone (occipital bone) and compressing the brainstem/cranial cervical spinal cord.

Note the bone fragment displaced cranially and compressing the brain stem.
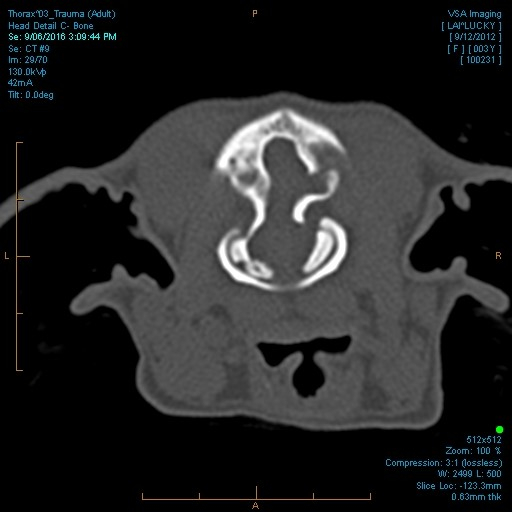
Note the fractured occipital condyle on the left and the right foramen fracture.
After a detailed discussion with Vicky it was decided to take Lucky to surgery with the goal of decompression of the brain/spinal cord and stabilisation of the atlanto-occipital joint. At surgery (Drs Jerram and Walker) we identified a large displaced piece of bone compressing the spinal cord. This was removed and the base of the brain (cerebellum) was decompressed by careful removal of some more of the occipital bone. Once the decompression was achieved Lucky’s head was then positioned in a normal standing position and stabilisation between the skull and the dorsal aspect of the C1 vertebra was performed by creating a custom device using titanium mesh and self tapping screws. Five screws were placed in the dorsal arch of the C1 vertebra and six screws were placed in the transverse sinus region of the skull. Following completion of this procedure, the skull and the C1 vertebra moved together (see radiograph below).

Lucky was placed in a neck splint and immediately showed improvement in the post-op period – marked reduction in pain when manipulated and stronger motor movement. Lucky could ambulate with assistance within one week and was walking strongly within a month. Lucky is still wearing the neck brace at 6 weeks post-op because she is trying to run around and is nearly normal neurologically.
This case demonstrates the huge advantage to having access to an in-hospital CT and without that equipment this life-saving surgery would not have been possible.
Thank you to Vicky for letting us tell Lucky’s story.
